
When your doctor orders pulmonary function tests, it’s not just a routine check. It’s a window into how well your lungs are actually working - especially when you’re short of breath, coughing often, or struggling to keep up during daily activities. Two of the most important tests in this group are spirometry and DLCO. Together, they tell a complete story: one measures airflow, the other measures how well oxygen moves from your lungs into your blood. But interpreting them isn’t as simple as reading numbers. You need to understand what the patterns mean - and what they don’t.
What Spirometry Really Measures
Spirometry is the most common lung test you’ll ever have. You blow into a tube as hard and fast as you can after taking the deepest breath possible. The machine records two key numbers: FEV1 (how much air you can force out in the first second) and FVC (how much you can blow out total). Then it calculates the ratio: FEV1 divided by FVC. Normal values? Usually above 80% of what’s predicted for your age, height, sex, and ethnicity. But here’s what matters more than the exact number: the pattern. If your FEV1/FVC ratio is below 0.7, that’s a classic sign of obstruction - meaning your airways are narrowed. Think asthma, COPD, or chronic bronchitis. Your lungs aren’t emptying properly. The air gets trapped. If both FEV1 and FVC are low, but the ratio is normal or even high, that’s restriction. Your lungs can’t expand fully. This could be due to scar tissue (like in pulmonary fibrosis), weak chest muscles, or even severe obesity. But here’s the trap: sometimes, severe air trapping from asthma or emphysema makes FVC look low - mimicking restriction. That’s where spirometry alone fails. You need DLCO to see the real picture.What DLCO Tells You That Spirometry Can’t
DLCO stands for diffusing capacity of the lung for carbon monoxide. It sounds technical, but it’s really about one thing: how well oxygen crosses from your lungs into your bloodstream. You inhale a tiny, harmless amount of carbon monoxide mixed with helium and oxygen. You hold your breath for exactly 10 seconds. Then you exhale. The machine measures how much CO was absorbed - which tells doctors how efficiently your alveoli (the tiny air sacs) and capillaries are working. Normal DLCO? Between 75% and 140% of predicted. But the real power of DLCO comes from how it compares to spirometry. If you have low FVC and low DLCO, it’s likely true lung restriction - like pulmonary fibrosis. The scar tissue thickens the barrier between air and blood, so oxygen can’t get through. But if you have low FVC and normal DLCO? That’s probably not lung damage. It’s something like scoliosis or obesity - the lungs are physically squeezed, but the gas exchange itself is fine. DLCO is also the first test to drop in early interstitial lung disease - often months or even years before spirometry shows any change. That’s why it’s critical for catching diseases like IPF (idiopathic pulmonary fibrosis) early.When DLCO Is High - And Why It Matters
Most people assume low DLCO is the only concern. But high DLCO can be just as telling. If your DLCO is above 140%, it could mean:- You’re having an asthma attack - your lungs are over-inflated and blood flow is increased
- You have polycythemia - too many red blood cells, so more CO gets absorbed
- You have a heart shunt - blood bypasses the lungs and picks up extra CO
- You’re bleeding into your lungs (pulmonary hemorrhage)
The FVC/DLCO Ratio: A Hidden Diagnostic Tool
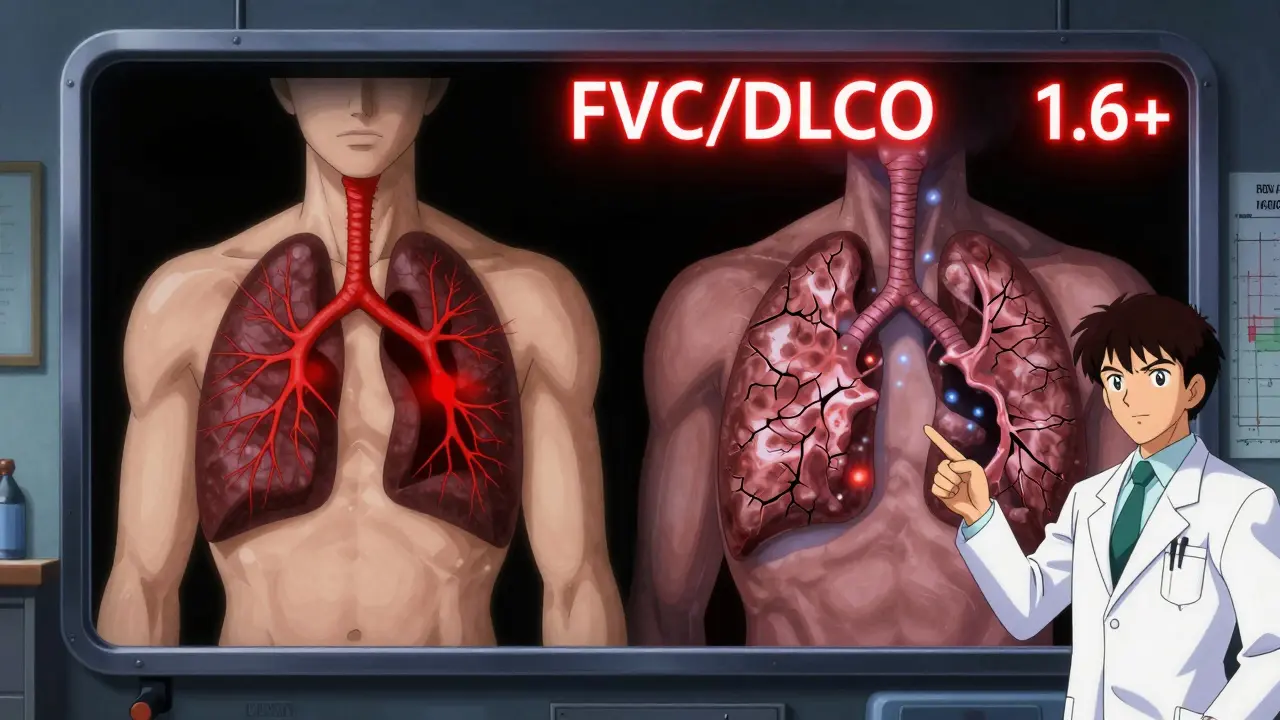
Most patients never hear about this number - but it’s one of the most powerful clues in pulmonary medicine. Take your FVC (from spirometry) and divide it by your DLCO. If the result is above 1.6, it’s a red flag for pulmonary hypertension - high blood pressure in the lungs. Why? Because in pulmonary hypertension, the small blood vessels in the lungs narrow or stiffen. Oxygen transfer drops (low DLCO), but lung volume stays normal or even increases (normal or high FVC). The ratio shoots up. Studies show this ratio is above 1.6 in over 90% of people with pulmonary hypertension. That’s more reliable than many imaging tests.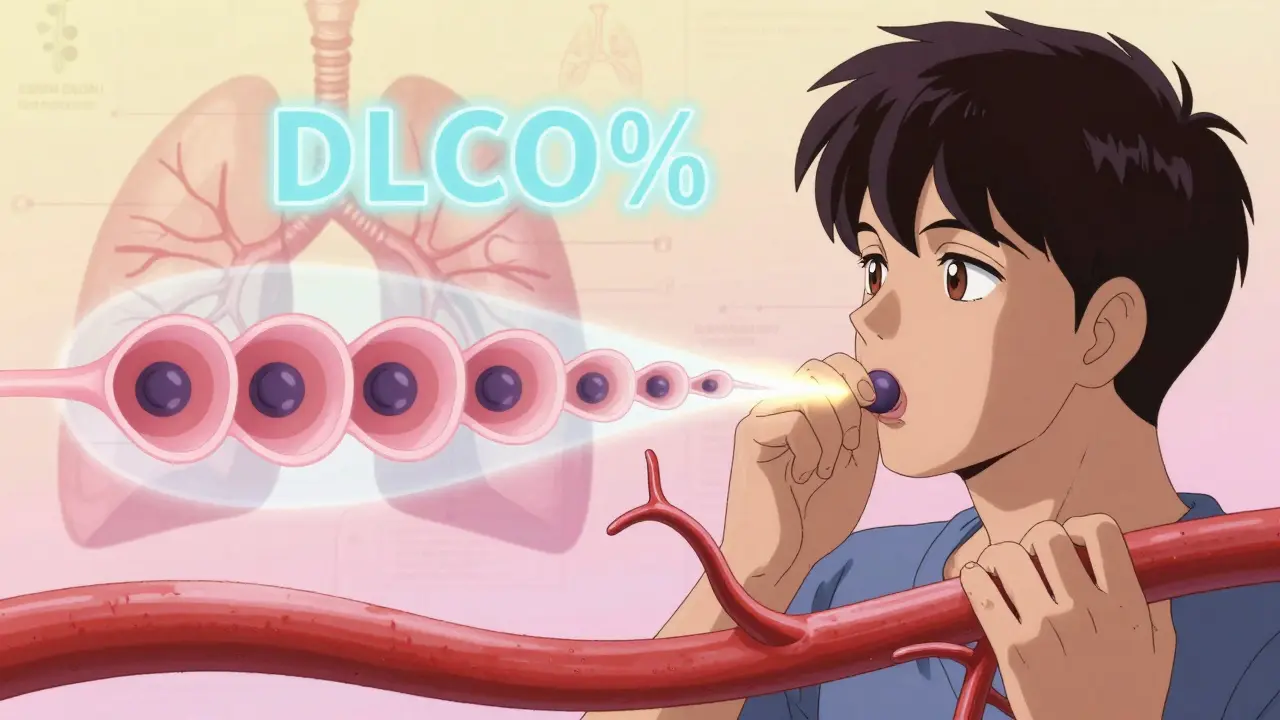
Why DLCO Is Often Misunderstood
Even among doctors, DLCO is the most overlooked test. Why? First, it’s harder to perform. Holding your breath for 10 seconds sounds easy - until you’re wheezing, elderly, or out of shape. About 15% of patients can’t do it properly. Second, it’s sensitive to things you might not think of:- Anemia: For every 1 g/dL drop in hemoglobin, DLCO falls about 1%. If your blood count is low, your DLCO looks worse than it is.
- Smoking: Carbon monoxide from cigarettes binds to hemoglobin, making your DLCO look artificially low - even if your lungs are fine.
- Altitude: At higher elevations, DLCO naturally drops because there’s less oxygen in the air.
What the Numbers Mean in Real Conditions
Let’s look at real-world examples:- Emphysema: FEV1/FVC low, FVC normal or low, DLCO very low - even if spirometry looks only mildly abnormal. DLCO is often the first sign.
- Pulmonary fibrosis: FVC low, FEV1/FVC normal or high, DLCO much lower than FVC. In advanced cases, DLCO can drop to 20-30% of predicted - while FVC is still at 60%. That’s how you know it’s serious.
- Chronic pulmonary embolism: Normal spirometry, but DLCO low. This is a classic trap. People think their lungs are fine - but they’re missing clots blocking blood flow.
- Asthma: Spirometry may be normal between attacks. DLCO is often normal or even high. If you have symptoms but normal spirometry and DLCO, your doctor might need to do a bronchoprovocation test.
When to Ask for DLCO - Even If Spirometry Is Normal
Don’t wait for abnormal spirometry to request DLCO. Ask for it if:- You have unexplained shortness of breath
- You’re being evaluated for lung surgery
- You have a connective tissue disease like scleroderma or rheumatoid arthritis
- You’ve been exposed to dust or chemicals (asbestos, silica)
- Your oxygen levels are low, but your chest X-ray looks fine
What Comes Next After the Tests
Once you have your results, don’t just look at the percentages. Look at the pattern. - Obstructive + low DLCO? Think emphysema or cystic fibrosis. CT scan needed. - Restrictive + low DLCO? Likely fibrosis. Referral to a lung specialist is urgent. - Restrictive + normal DLCO? Probably mechanical - check posture, weight, or spine. - Normal spirometry + low DLCO? Rule out pulmonary embolism, early fibrosis, or heart disease. If your doctor doesn’t explain the pattern - ask. If they don’t mention DLCO when you have symptoms - ask why. This isn’t just a test. It’s a diagnostic tool that can catch life-threatening conditions before they become irreversible.What’s Changing in 2025
New guidelines from the American Thoracic Society and European Respiratory Society now require hemoglobin correction for every DLCO test. That’s standard practice - but not yet universal. AI tools are starting to help. A 2023 Mayo Clinic study showed algorithms could predict pulmonary hypertension from DLCO patterns with 88% accuracy - faster and cheaper than right heart catheterization. And reimbursement? DLCO is now covered by Medicare at $85-$110 per test. That’s up from $70 in 2020. More clinics are offering it because the value is clear.Final Takeaway
Spirometry tells you if your airways are blocked. DLCO tells you if your lungs can deliver oxygen to your body. One is about flow. The other is about function. Most people think if they can blow hard, their lungs are fine. That’s wrong. You can have normal spirometry and still have a serious lung problem - if the gas exchange is failing. If you’ve been told your lungs are “normal” but you’re still struggling to breathe - ask for DLCO. It might be the only test that sees what’s really going on.What’s the difference between spirometry and DLCO?
Spirometry measures how much air you can move in and out of your lungs and how fast - it’s about airflow. DLCO measures how well oxygen moves from your lungs into your bloodstream - it’s about gas exchange. One looks at the pipes, the other looks at the transfer of oxygen.
Can DLCO be normal if I have emphysema?
Yes - but only in very early stages. Emphysema destroys the air sacs and capillaries, so DLCO usually drops early - often before spirometry shows changes. A normal DLCO doesn’t rule out emphysema, but a low DLCO with normal spirometry is a major red flag. A CT scan is needed to confirm.
Why does my hemoglobin level matter for DLCO?
Carbon monoxide in the test binds to hemoglobin in your blood. If you’re anemic (low hemoglobin), less CO gets absorbed - so your DLCO looks lower than it should. A drop of 1 g/dL in hemoglobin can lower DLCO by about 1%. Always check your blood count before interpreting DLCO.
Can smoking affect my DLCO results?
Yes. Smoking increases carbon monoxide in your blood, which competes with the test gas. This can falsely lower your DLCO by 5-10%. If you smoke, your doctor should wait at least 24 hours after your last cigarette before testing - and ideally, you should quit.
Is a low DLCO always serious?
Not always - but it always needs investigation. Low DLCO can mean anything from early pulmonary fibrosis to chronic blood clots in the lungs, heart failure, or even anemia. It’s not a diagnosis - it’s a signal. The pattern with your spirometry and symptoms tells the real story.
Should I get a DLCO if my spirometry is normal?
Yes - if you have ongoing shortness of breath, a history of lung exposure (like dust or asbestos), or a connective tissue disease like lupus or scleroderma. DLCO can detect early lung damage years before spirometry changes. Normal spirometry doesn’t mean normal lungs.
Mark Able
December 17, 2025 AT 14:23Bro I had this test last month and my DLCO was 58% but my spirometry was fine. Doc just shrugged and said 'probably just aging' - yeah right. I've been coughing for 18 months and my oxygen sat drops when I walk to the fridge. I asked for a CT and they laughed. Now I'm seeing a pulmonologist on my own dime. Don't let them gaslight you.
James Stearns
December 19, 2025 AT 03:14One must observe that the conflation of pulmonary function metrics with clinical symptomatology constitutes a fundamental epistemological oversight in contemporary respiratory diagnostics. The reductionist paradigm of FEV1/FVC ratio as a diagnostic proxy neglects the ontological complexity of alveolar-capillary membrane dynamics. Furthermore, the assertion that DLCO is 'the only test' capable of detecting early interstitial disease is empirically unsound, as high-resolution computed tomography remains the gold standard for structural assessment. One is compelled to question the pedagogical rigor of such oversimplifications.
Nina Stacey
December 20, 2025 AT 11:50omg this is so helpful i’ve been struggling with breathlessness for years and my doctors always say ‘your lungs look fine’ but i know something’s off and this totally explains why i need the dlco test too i had no idea anemia could mess with the results and i’m on iron supplements now wow this just clicked for me thank you so much for writing this 🙏
Kinnaird Lynsey
December 21, 2025 AT 02:30Interesting. I’ve seen a lot of patients with normal spirometry and low DLCO - mostly former smokers with no COPD diagnosis. The real kicker? Most of them don’t even know they’re supposed to stop smoking before the test. I’ve had results skewed by last night’s cigarette more times than I can count. Funny how the simplest things get overlooked.
Andrew Kelly
December 22, 2025 AT 15:41Who funds these guidelines? Big Pharma? DLCO costs $100 and they’re pushing it like it’s a miracle cure. Meanwhile, the real cause of most breathing issues is air pollution, stress, and poor posture - not some magical gas exchange failure. And why is no one talking about how many people can’t hold their breath for 10 seconds because they’re 70 and out of shape? This test is a scam for people who can’t admit medicine is broken.
Moses Odumbe
December 22, 2025 AT 21:21DLCO = oxygen transfer 🫁💨
spirometry = air flow 🌬️
you need both
if one’s off, don’t ignore it
if both are off, run 😱
also anemia = fake low DLCO 🤯
smoking = fake low DLCO 🚬
altitudes = fake low DLCO 🏔️
if your doc doesn’t check hemoglobin, find a new one. 💪
Vicki Belcher
December 23, 2025 AT 13:14This is the most clear explanation I’ve ever read. I work in a clinic and we used to skip DLCO unless it was ‘obvious’ - now I’m telling every patient with unexplained dyspnea to ask for it. Also, the FVC/DLCO ratio >1.6 for pulmonary hypertension? Mind blown. I just ordered one for my 68-year-old patient with no cough, normal X-ray, and 100% oxygen saturation. She’s been told she’s ‘just old’ for three years. This might change everything. 🙌
anthony funes gomez
December 23, 2025 AT 17:43The diagnostic utility of DLCO, when contextualized within the broader framework of ventilatory mechanics and perfusion dynamics, reveals a critical epistemic gap in primary care pulmonary evaluation - particularly when confounding variables - hemoglobin concentration, ambient atmospheric pressure, and exogenous CO exposure - are not systematically corrected for, thereby rendering the metric non-comparable across populations, and thus, clinically unreliable unless standardized. The current trend toward algorithmic interpretation, while statistically compelling, risks reifying a reductionist paradigm that neglects the phenomenological experience of dyspnea - a phenomenon not reducible to numerical indices. One must ask: Is the test measuring physiology - or merely statistical deviation?