When someone starts forgetting names or losing their way home, the first thought for most people is Alzheimer's disease. It’s the name everyone knows. But here’s the thing: Alzheimer’s is just one piece of a much larger puzzle. In fact, about 35 to 40 percent of all dementia cases worldwide are caused by other conditions entirely. Three of the most common-and often misunderstood-are vascular dementia, frontotemporal dementia (FTD), and Lewy body dementia (LBD).
Knowing which type you’re dealing with isn’t just an academic exercise. It changes everything. The treatment for one can be dangerous for another. The care strategies differ wildly. And the timeline for progression? That varies too. If you’ve been told a loved one has “dementia” but nothing else, you’re missing half the picture. Let’s break down these three distinct conditions so you know what to look for, what to ask doctors, and how to navigate the path ahead.
Vascular Dementia: When Blood Flow Fails
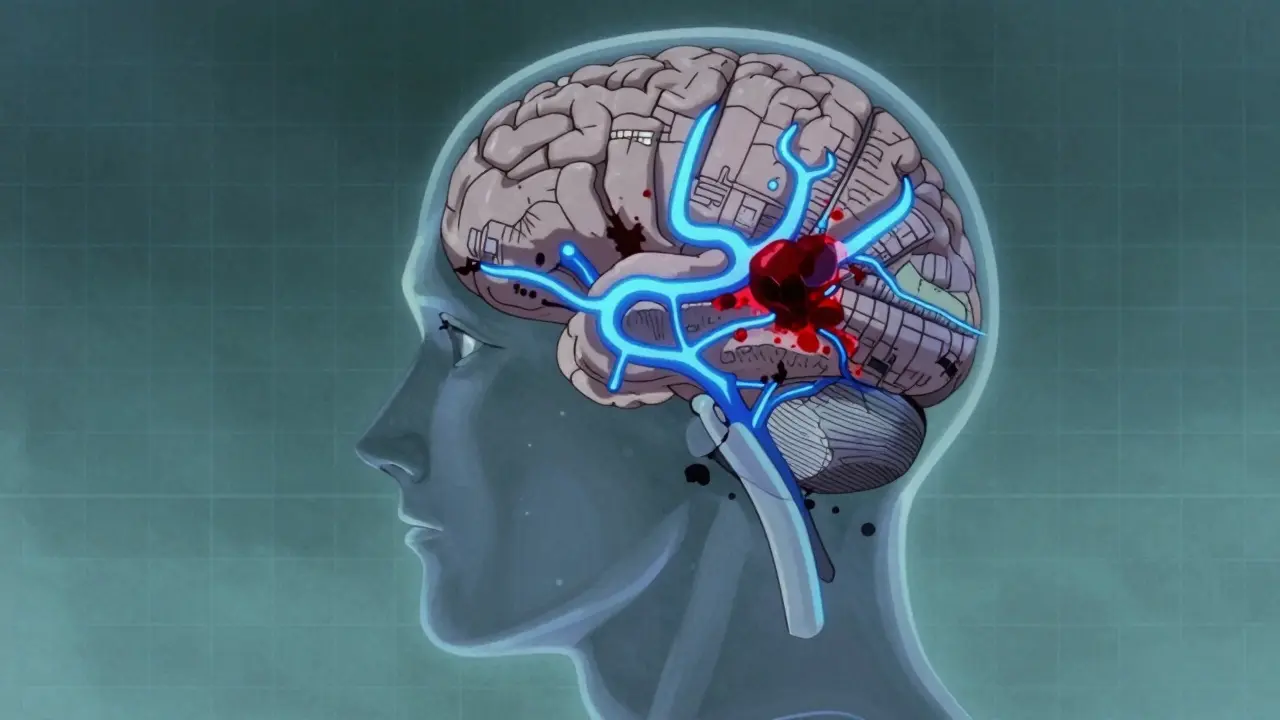
Vascular dementia is exactly what it sounds like: brain damage caused by problems with blood flow. Imagine your brain as a city. If the roads get blocked by debris-blood clots, plaque, or burst vessels-the neighborhoods downstream suffer. In medical terms, this means parts of the brain die because they aren’t getting enough oxygen.
This is the second most common form of dementia, accounting for roughly 10 percent of cases. Unlike Alzheimer’s, which creeps in slowly like fog, vascular dementia often hits in steps. A person might seem fine for months, then suddenly decline after a small stroke or a transient ischemic attack (TIA). You might notice them struggling to follow instructions, misplacing items frequently, or having trouble planning simple tasks.
The key difference here is that movement and coordination issues show up earlier than in Alzheimer’s. Walking might become shuffling, balance could wobble, and judgment takes a hit. Because it’s tied to heart health, managing vascular dementia is largely about managing risk factors. High blood pressure, diabetes, and high cholesterol are the enemies. Doctors typically prescribe medications to lower blood pressure (aiming for under 130/80 mmHg), control blood sugar, and prevent clots with antiplatelets like aspirin.
If you suspect vascular dementia, brain imaging is crucial. An MRI or CT scan will show the scars of past strokes or areas where blood flow has been compromised. Early detection matters because preventing further vascular events can slow the decline significantly.
Frontotemporal Dementia: The Personality Shift
Now, let’s talk about the one that often gets mistaken for a midlife crisis or a psychiatric disorder. Frontotemporal dementia (FTD) affects the frontal and temporal lobes-the parts of the brain responsible for personality, behavior, language, and reasoning. It’s rare compared to Alzheimer’s, making up only about 10 percent of cases, but it’s the most common dementia in people under 60.
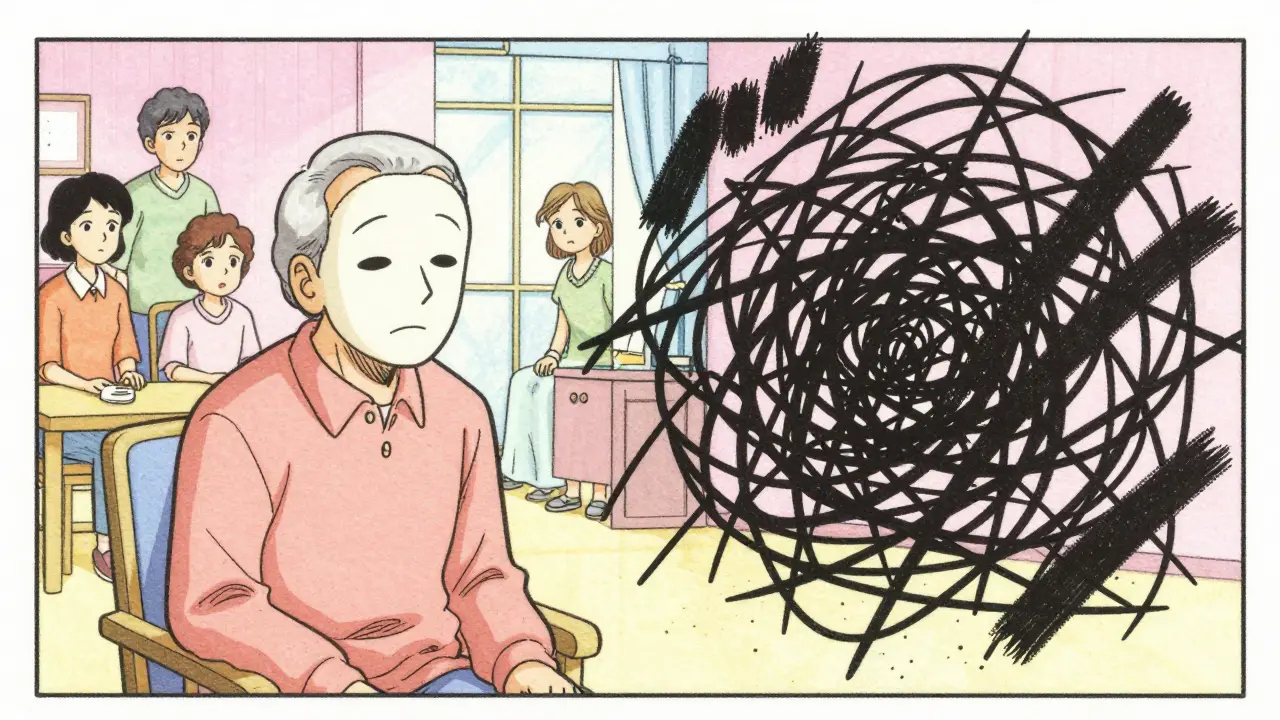
Here’s the kicker: memory often stays sharp in the early stages. Instead, you’ll see dramatic changes in behavior. A once cautious person might become impulsive, spending money recklessly or acting in socially inappropriate ways. Someone who was always warm and engaged might become emotionally flat, showing no interest in family or hobbies. Conversely, some become excessively emotional or aggressive.
Language problems are also a hallmark. People with FTD might struggle to find words, repeat phrases endlessly, or lose the ability to understand speech altogether. This variant is sometimes called primary progressive aphasia. Movement issues can creep in later, including shaky hands or difficulty walking.
Diagnosing FTD is tricky. Up to 50 percent of cases are initially misdiagnosed as depression, bipolar disorder, or schizophrenia. Doctors rely on MRI scans showing shrinkage in the frontal and temporal lobes, along with neuropsychological tests that focus on executive function rather than memory. There’s no cure for FTD, and standard Alzheimer’s drugs don’t work. Treatment focuses on managing symptoms, often using SSRIs to help with mood and behavior, and speech therapy for language difficulties.
Lewy Body Dementia: The Fluctuating Fog
Lewy body dementia (LBD) is perhaps the most complex of the three. It’s characterized by abnormal protein deposits called Lewy bodies in the brain. These proteins disrupt thinking, movement, and behavior. LBD accounts for 15 to 20 percent of dementia cases, affecting around 1.4 million Americans alone.
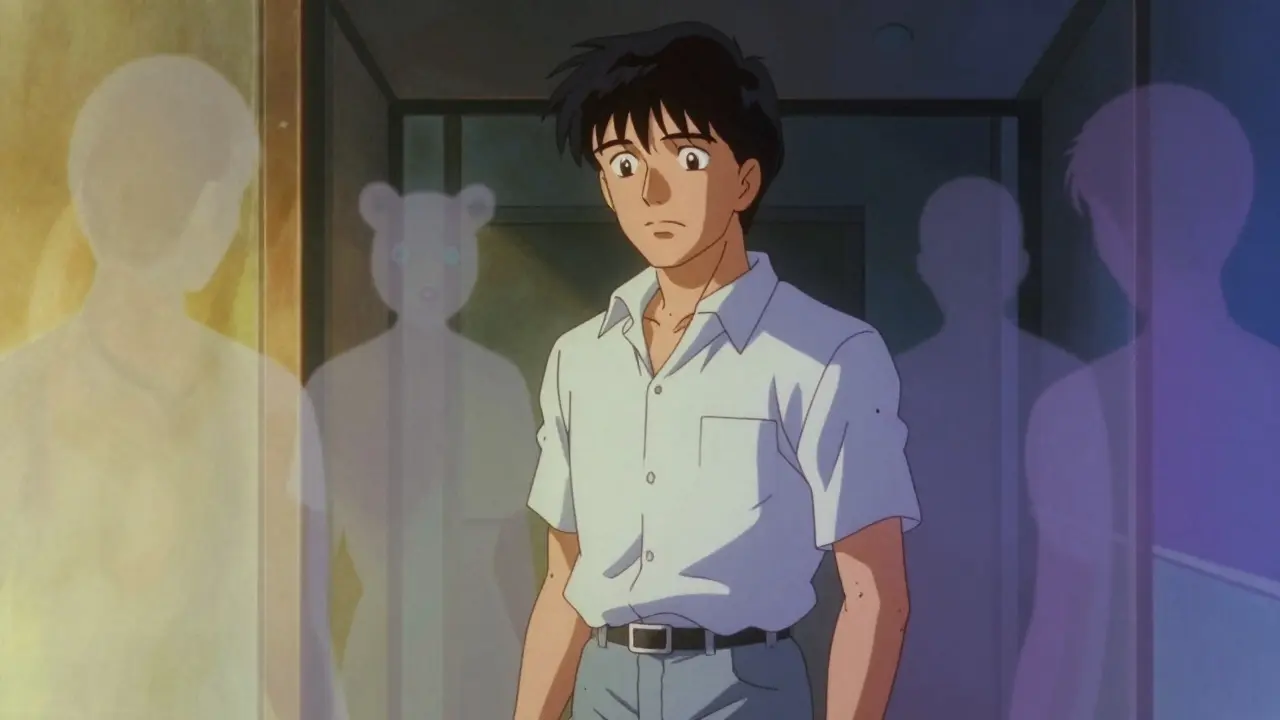
The defining feature of LBD is fluctuation. One hour, your loved one might be alert, conversant, and clear-headed. The next, they’re confused, drowsy, or staring into space. These shifts can happen daily or even hourly. Visual hallucinations are another core symptom. They might see children, animals, or strangers in the room. Importantly, these visions are usually not frightening to the person experiencing them, though they can be unsettling for caregivers.
Movement problems mimic Parkinson’s disease: stiffness, tremors, slow walking, and a masked facial expression. Sleep disturbances are also common, particularly REM sleep behavior disorder, where people act out their dreams-kicking, punching, or shouting while asleep.
Here’s why accurate diagnosis is critical: LBD patients are extremely sensitive to antipsychotic medications. Drugs commonly used to treat agitation in Alzheimer’s can cause severe reactions in LBD, including worsening parkinsonism, extreme sedation, or even life-threatening conditions. Instead, doctors may prescribe cholinesterase inhibitors like rivastigmine to help with cognition and attention. Misdiagnosis is rampant; up to 75 percent of LBD cases are initially labeled as Alzheimer’s.
Comparing the Three: What Sets Them Apart?
| Feature | Vascular Dementia | Frontotemporal Dementia (FTD) | Lewy Body Dementia (LBD) |
|---|---|---|---|
| Primary Cause | Reduced blood flow/strokes | Tau/TDP-43 protein buildup | Alpha-synuclein (Lewy bodies) |
| Onset Pattern | Sudden, step-wise decline | Gradual behavioral/language change | Fluctuating cognition |
| Early Symptoms | Planning issues, movement problems | Personality shift, impulsivity | Visual hallucinations, sleep disorders |
| Memory Loss | Present, but variable | Often preserved early on | Less prominent early on |
| Typical Age | 65+ | 40-65 (youngest onset) | 50+ |
| Medication Caution | Manage blood pressure/sugar | Avoid standard Alzheimer’s drugs | Avoid antipsychotics |
Why Diagnosis Matters More Than Ever
You might wonder, “Does it really matter if we just call it dementia?” Yes, it matters immensely. Consider medication. If you give a typical antipsychotic to someone with Lewy Body Dementia to calm agitation, you could trigger a severe neurological reaction. For Vascular Dementia, ignoring high blood pressure guarantees more brain damage. For FTD, treating it as depression delays proper support for behavioral crises.
Diagnostic tools have improved. For LBD, DaTscan imaging can detect dopamine transporter deficits with high accuracy. For FTD, FDG-PET scans show reduced metabolism in specific brain regions. For Vascular Dementia, the Fazekas scale helps quantify white matter damage on MRIs. Pushing for a specific diagnosis isn’t nitpicking; it’s ensuring safety and appropriate care.
Caregiver education is also type-specific. Knowing that LBD hallucinations are visual and often harmless prevents unnecessary panic. Understanding that FTD apathy isn’t laziness but brain damage fosters patience. Recognizing that Vascular Dementia risks are linked to heart health empowers proactive management.
Next Steps for Families and Caregivers
If you’re navigating this terrain, start by documenting symptoms. Note when confusion happens, what triggers behavioral changes, and any physical symptoms like tremors or sleep issues. Bring this log to a neurologist or geriatric specialist. Ask specifically about vascular risk factors, behavioral variants, and Lewy body features.
Don’t accept a vague “it’s just old age” answer. Seek a second opinion if the first doctor dismisses your concerns. Join support groups specific to the type of dementia. The experiences of families dealing with FTD are vastly different from those coping with LBD, and targeted advice is invaluable.
Finally, prioritize prevention where possible. For vascular dementia, controlling hypertension and diabetes can reduce risk by up to 20 percent. While there’s no cure for FTD or LBD yet, early diagnosis allows for better symptom management and planning. Research is advancing, with new biomarkers and trials targeting specific proteins like alpha-synuclein and tau. Staying informed keeps you empowered.
Can vascular dementia be reversed?
No, existing brain damage cannot be reversed. However, preventing further strokes through strict blood pressure and diabetes management can halt or slow progression significantly.
Is frontotemporal dementia hereditary?
About 30 percent of FTD cases have a genetic link. If multiple family members are affected, genetic counseling may be recommended to identify mutations like C9orf72.
What should I do if my loved one with LBD sees things?
Stay calm and reassure them. Do not argue about the reality of the hallucination. Ensure the environment is well-lit to reduce shadows that might trigger visions. Never use antipsychotic meds without explicit neurologist approval.
How long does each type last?
Varies widely. Vascular dementia depends on stroke frequency. FTD averages 6-8 years. LBD typically lasts 5-8 years after diagnosis, though individual outcomes depend on overall health and complications.
Are Alzheimer’s drugs safe for these types?
Generally no. Cholinesterase inhibitors may help LBD but can worsen FTD. They offer little benefit for pure vascular dementia. Always consult a specialist before starting any cognitive enhancers.