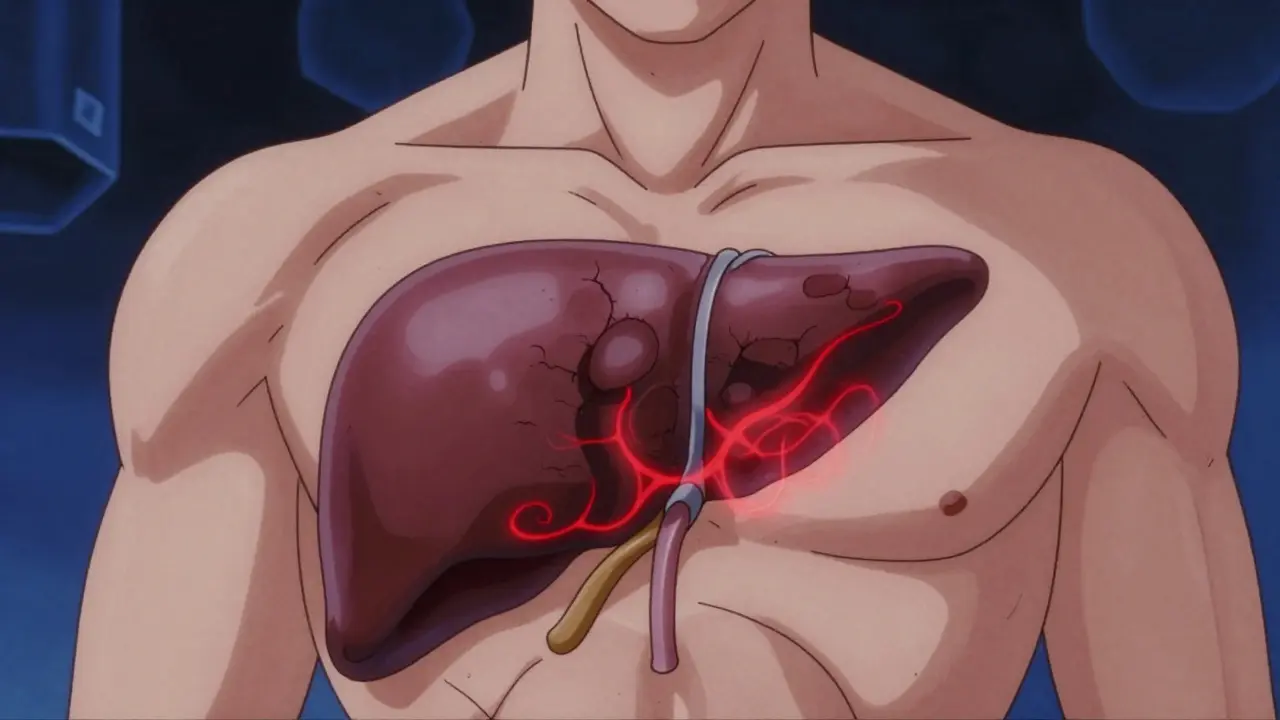
Imagine your liver turning against you. Instead of filtering toxins, it becomes a hardened, scarred organ that blocks blood flow and struggles to keep you alive. This is Cirrhosis, the irreversible end-stage of chronic liver disease characterized by extensive fibrosis and architectural distortion. It is not just a diagnosis; it is a life-altering condition that affects approximately 600,000 Americans. While the scarring itself cannot be undone, understanding how to manage the complications can mean the difference between a stable life and a crisis.
The journey with cirrhosis is often divided into two phases: compensated and decompensated. In the compensated stage, you might feel fine or experience only mild fatigue. But once the liver function drops significantly, you enter the decompensated stage. This is when serious complications arise. The goal of modern management is not just to treat symptoms but to prevent these events from happening in the first place, or to catch them early enough to avoid hospitalization.
Understanding the Warning Signs: From Fatigue to Jaundice
Many people walk around with cirrhosis for years without knowing it because the liver is incredibly resilient. However, as damage accumulates, specific signs emerge. You might notice extreme tiredness that sleep doesn’t fix. According to data from the University of Miami Health System, about 72% of patients report significant fatigue. Others experience unintentional weight loss or easy bruising because the liver stops producing enough clotting factors.
As the disease progresses, the signs become harder to ignore. Yellowing of the skin and eyes (jaundice) occurs when bilirubin builds up in the blood. Swelling in the legs (edema) and abdomen (ascites) happens because fluid leaks out of blocked blood vessels. If you start feeling confused, having trouble concentrating, or experiencing "brain fog," this could be hepatic encephalopathy-a buildup of toxins affecting the brain. Recognizing these changes early allows doctors to intervene before they become emergencies.
Portal Hypertension and Ascites: Managing Fluid Buildup
One of the most common and distressing complications is ascites, which is fluid accumulation in the abdomen. It stems from portal hypertension-high pressure in the vein that carries blood from the intestines to the liver. When scar tissue blocks this flow, pressure rises, forcing fluid into the abdominal cavity. About half of all cirrhosis patients develop ascites within ten years of diagnosis.
Managing ascites starts with diet. You need to restrict sodium intake to less than 2 grams per day. This isn't just about skipping the salt shaker; it means avoiding processed foods, canned soups, and fast food. Diuretics, often called water pills, are the next step. Doctors typically prescribe spironolactone and furosemide together. Most people respond well to this combination. However, if the fluid returns quickly despite medication, you may have refractory ascites. In these cases, large-volume paracentesis-a procedure to drain the fluid with a needle-is necessary. To prevent shock after draining large amounts of fluid, doctors infuse albumin, a protein that helps maintain blood volume.
| Scoring System | Parameters Used | Primary Use Case | Precision Level |
|---|---|---|---|
| Child-Pugh-Turcotte | Bilirubin, Albumin, INR, Ascites, Encephalopathy | General prognosis and surgical risk assessment | Moderate (Class A, B, C) |
| MELD Score | Serum Creatinine, Bilirubin, INR | Liver transplant priority allocation | High (Numerical score) |
| FibroScan | Liver stiffness measurement (kPa) | Non-invasive diagnosis of fibrosis/cirrhosis | High (>12.5 kPa indicates cirrhosis) |
Hepatic Encephalopathy: Clearing the Brain Fog
When the liver fails to filter ammonia and other toxins from the blood, these substances travel to the brain. This causes hepatic encephalopathy. Symptoms range from mild confusion and sleep disturbances to severe disorientation and coma. It affects 30-45% of patients with decompensated cirrhosis.
The standard treatment involves lactulose, a syrup that helps pull ammonia out of the body through bowel movements. The goal is to achieve two to three soft stools per day. While effective, lactulose can cause bloating and diarrhea, which many patients find socially difficult. For those who still have episodes, doctors add rifaximin, an antibiotic that reduces toxin-producing bacteria in the gut. Studies show that combining rifaximin with lactulose cuts hospitalizations for encephalopathy by nearly 60%. It is crucial to take these medications consistently, even when you feel fine, to prevent sudden flare-ups.
Preventing Bleeding: Varices and Beta-Blockers
Portal hypertension doesn't just push fluid into the abdomen; it also forces blood into smaller veins in the esophagus and stomach. These veins swell and become fragile, known as varices. If a varix bursts, it causes massive, life-threatening bleeding. About 30% of cirrhosis patients will experience a variceal bleed at some point.
To prevent this, doctors use non-selective beta-blockers like nadolol or propranolol. These drugs lower the pressure in the portal vein, reducing the risk of bleeding by 45%. Another option is carvedilol, which has shown superior pressure reduction in recent studies. Additionally, regular upper endoscopies are essential. During this procedure, a doctor can see the varices and tie them off with rubber bands (endoscopic band ligation) before they rupture. If you ever vomit blood or have black, tarry stools, seek emergency care immediately.
Cancer Surveillance: Catching Hepatocellular Carcinoma Early
Cirrhosis significantly increases the risk of hepatocellular carcinoma (HCC), the most common type of liver cancer. The risk is about 2-8% per year. Because early-stage liver cancer often has no symptoms, surveillance is critical. Guidelines recommend an ultrasound every six months for all patients with cirrhosis.
This screening detects tumors while they are small and potentially curable. If caught early, options include surgery, ablation, or transplantation. Without screening, cancers are often found at advanced stages where treatment is limited. Do not skip these appointments. They are one of the most powerful tools you have to extend your life.
Treatment Advances and Transplant Criteria
Medical science is making strides in treating the underlying causes of liver damage. For hepatitis C, direct-acting antivirals can cure the infection in over 95% of cases, stopping further damage. Recently, the FDA approved resmetirom for metabolic dysfunction-associated steatohepatitis (MASH), showing promise in improving fibrosis. However, if the liver is too damaged, these treatments cannot reverse existing cirrhosis.
In such cases, a liver transplant may be the only option. The decision to list a patient for transplant is based on the MELD score, which predicts short-term mortality. A score of 15 or higher generally qualifies you for evaluation. The system recently updated to include quality-of-life metrics, recognizing that suffering matters as much as lab values. While wait times can be long, living donor transplants offer a faster alternative for some. Success rates are high, with many patients returning to work and normal activities within a year.
Daily Management: Nutrition and Lifestyle
Living with cirrhosis requires daily vigilance. Nutrition plays a huge role. Contrary to old advice, you do not need to restrict protein unless you have severe, uncontrolled encephalopathy. In fact, malnutrition is a major risk. Aim for small, frequent meals throughout the day, including a late-night snack to prevent muscle breakdown. Work with a dietitian to ensure you get enough calories and nutrients.
Avoid alcohol completely. Even small amounts can accelerate liver failure. Be cautious with medications, including over-the-counter pain relievers like ibuprofen, which can worsen kidney function and bleeding risks. Acetaminofen is usually safe in limited doses (under 2g/day), but always check with your doctor. Monitor your weight daily to detect fluid retention early. Sudden weight gain often signals worsening ascites.
Can cirrhosis be reversed?
Established cirrhosis is considered irreversible due to permanent scarring. However, treating the underlying cause (like curing hepatitis C or stopping alcohol use) can prevent further damage and allow the liver to function better. New therapies like resmetirom show potential for improving fibrosis in specific conditions, but they do not fully reverse established cirrhosis.
What is the average life expectancy with cirrhosis?
Life expectancy varies widely depending on whether the cirrhosis is compensated or decompensated. Patients with compensated cirrhosis can live for decades. Once decompensation occurs, the median survival without transplant is about 2-3 years, though this improves significantly with proper management of complications like ascites and varices.
How does the MELD score affect transplant priority?
The Model for End-Stage Liver Disease (MELD) score calculates the severity of your illness based on blood tests (bilirubin, creatinine, INR). Higher scores indicate sicker patients and result in higher priority for liver transplants. A score of 15 or above typically qualifies you for the national waiting list, with higher numbers moving you up the queue faster.
What foods should I avoid with cirrhosis?
You must strictly limit sodium (salt) to under 2 grams per day to manage fluid buildup. Avoid processed meats, canned goods, and restaurant foods which are high in hidden salt. Also, avoid raw seafood due to infection risks, and limit alcohol completely. Protein restriction is rarely needed unless you have severe hepatic encephalopathy.
When should I go to the emergency room?
Seek immediate care if you experience vomiting blood, black tarry stools, severe abdominal pain, fever with chills, or sudden confusion/drowsiness. These are signs of variceal bleeding, spontaneous bacterial peritonitis, or severe hepatic encephalopathy, all of which are medical emergencies requiring urgent intervention.